Pharmacy Benefit Manager (PBM) Reform
PBM Overview
Pharmacy Benefit Managers (PBMs) work with health insurers, large employers and other payers to manage prescription drug benefits. The initial role of PBMs was to negotiate reimbursement rates with drug manufacturers, manage prescription drug claims, and reimburse pharmacies for dispensed medications. Since its inception, the role of the PBMs have evolved over time to now being more complex, with multiple lines of business (eg, specialty pharmacies, mail-order pharmacies, and group purchasing). Today, PBMs play a central role in shaping patient access to medications by developing and managing formularies of covered drugs, which significantly impacts the application of utilization management strategies and patient cost-sharing requirements.
The PBM Problem: How Revenue Models May Drive Misaligned Incentives
PBMs generate revenue in several ways:
Another indirect way that PBMs generate additional revenue is by steering business to their specific pharmacies, which allows them to save on dispensing fees and pharmacy operations costs as well as capture revenue for high-cost drugs by limiting the networks to the pharmacies that they own. PBMs then reimburse other smaller, independent pharmacies at a lower rate.
While PBMs were intended to help control rising drug prices and patient costs through price negotiations and formulary management, many believe that their financial incentives have often driven the opposite effect.
Role of a Pharmacy Benefit Manager in Providing Services and Flow of Funds for Prescription Drugs
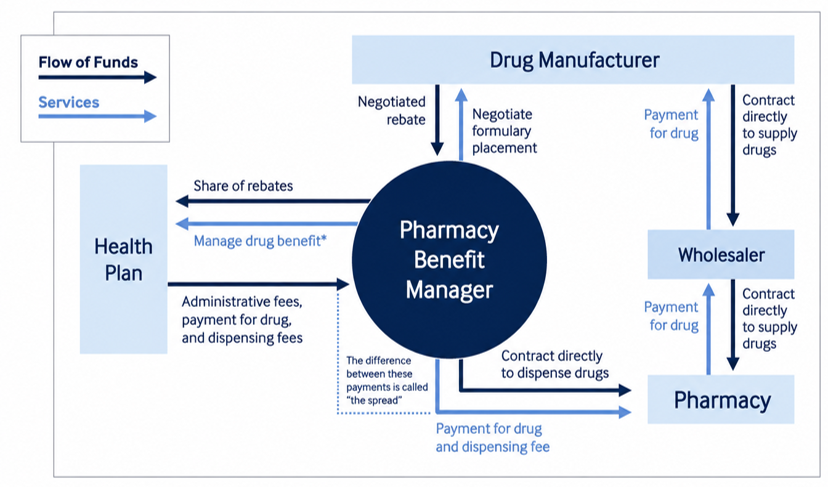
Includes establishing formulary and patient adherence programs and implementing utilization management tools, such as prior authorization, step therapy, and tiering, to steer patients toward certain drugs on formulary.
Data: Adapted from Congressional Budget Office, “Prescription Drug Pricing in the Private Sector” (CBO, Jan. 2007).
Source: Kristi Martin, “What Pharmacy Benefit Managers Do, and How They Contribute to Drug Spending” (explainer), Commonwealth Fund, Mar. 17, 2025.
https://doi.org/10.26099/fqag-v980
Key Issues Driving PBM Reform Today
In 2024, 24 states have taken action in the form of passing 33 bills aimed at regulating PBMs. Example legislation included prohibiting “spread pricing” and mandating that PBMs provide reports on the rebates that they receive. The momentum continues to grow in 2025, as more states have introduced legislation for PBM reform.
Other areas considered for PBM reform include:
Legal Challenges Targeting PBMs: Reform in Action
PBMs have faced more scrutiny in recent years, resulting in several lawsuits against PBMs; PBMs are also countersuing:
How Magnolia Market Access Can Support Manufacturers in Responding to PBM Reform
With the mounting pressure on the PBM industry, Magnolia can help you navigate the changing landscape and protect patient access through strategic, data-driven market access solutions. Here are several ways we support manufacturers in responding to PBM reform:
Partner with Magnolia Market Access
Contact us today to learn more about how we can support your market access strategy in this evolving environment. Our team is ready to help you stay ahead of PBM reforms and ensure sustainable access for your therapies
Related Content:
References:
- https://oversight.house.gov/wp-content/uploads/2024/07/PBM-Report-FINAL-with-Redactions.pdf
- https://www.commonwealthfund.org/publications/explainer/2025/mar/what-pharmacy-benefit-managers-do-how-they-contribute-drug-spending
- https://www.ftc.gov/terms/pharmacy-benefits-managers-pbm
- https://www.reuters.com/business/healthcare-pharmaceuticals/ftc-puts-hold-insulin-lawsuit-against-drug-middlemen-2025-04-02/
- https://www.fiercehealthcare.com/payers/pbms-strike-back-ftc-claim-administrative-process-unconstitutional
- https://www.fiercehealthcare.com/payers/express-scripts-files-suit-against-ftc-demands-retraction-report-pbm-industry
- https://ncpa.org/hp-pbms-are-docket-two-legal-fights-2024
- https://www.ajmc.com/view/goodrx-pbms-hit-by-price-fixing-lawsuits
- https://www.pharmacytimes.com/view/pbm-reform-takes-off-in-2025